Exposure and response prevention therapy, or ERP, is Mountain Valley’s core therapeutic approach. Often referred to simply as “exposure therapy,” this approach is largely what it sounds like—a systematic method of carefully but assertively exposing individuals to the everyday things that cause them outsized fear. Exposure therapy, when artfully implemented, essentially extinguishes the “fear of fear” that is at the core of most anxiety-based avoidance and dysfunction.
But to optimize and accelerate our use of exposure therapy, Mountain Valley utilizes a host of holistic, milieu-based approaches that are based on the highly practical orientation of mental-health occupational therapy. In this article, our executive program director, Zack Schafer, MS, OTR/L, introduces one aspect of this OT-informed program of care: sensory integration therapy.
Sensory integration therapy allows us to understand each resident’s unique sensory profile so that we can customize their exposures for maximum effectiveness. Our sensory work also provides residents with the insights and skills necessary to take charge of their own sensory processing and integration—i.e. their ability to understand and better regulate their own emotional responses. Since sensory processing difficulties predispose people to anxiety and related disorders, addressing these difficulties is a critical piece of the treatment puzzle at Mountain Valley.
What Is Sensory Integration Therapy?
Occupational Therapy (OT) has a long history with exploring the role of sensory system in human behavior. Dr. Jean Ayres, a clinical psychologist and occupational therapist, first founded Sensory Integration Therapy in the 1970’s. Her original theories, works, and practices have been applied, contested, and developed over the years. Nowadays, the use of sensory based strategies has become more prevalent in the treatment of a variety of psychiatric disorders. We see sensory strategies incorporated for emotional regulation in established therapy protocols, such as DBT TIPP skills. Occupational therapist, Tina Champagne developed her Sensory Modulation program which has been applied in a wide range of mental health institutions as means to reduce the use of seclusion and restraint. We even see sensory-motor approaches being applied in innovative trauma treatments, such as the Sensory Motor Arousal Regulation Treatment (SMART) approach developed in Bessel van der Kolk’s trauma center, by Elizabeth Warren and Andrea Koomar.
Sensory strategies have even gone “mainstream” and seem to be gaining popularity within the general public. We see fidget spinners in the classroom, pop-it’s on every kids back packs, and cozy weighted blankets advertised on Amazon.
But what exactly is sensory processing? How do sensory based interventions work? And what is the practical application of this knowledge for people who struggle with anxiety and OCD?
What Is Sensory Processing?
Let’s start by getting on the same page with a few “simple” definitions. Sensory Processing is one’s ability to perceive, modulate, and organize sensory input to create an adaptive response to one’s environment. In Jean Ayer’s original theory, she referred to this as Sensory Integration. She used the word integration to highlight the fact that we are always receiving a multitude of sensory stimuli, and our brain is engaged a very complex process of organizing this information effectively so we can engage with our environment adaptively. Although sensory integration was the original language used by Ayers, over the years the term sensory processing has become more common. You will often hear this the term used in ways such as “they have a sensory processing challenge,” or you may even hear that someone has a “sensory processing disorder” (*It’s important to acknowledge that despite how often you may hear the terms ‘sensory processing disorder” this is not a formal a diagnosis acknowledged by the American Psychiatric Association [APA]).
Sensory Discrimination & Sensory Modulation
For those who have sensory processing challenges, they often have challenges with two main components of sensory processing: sensory discrimination or sensory modulation. Sensory Discrimination is one’s ability to accurately perceive, identify, and conceptualize sensory input. Examples include one’s ability to accurately recognize their name when it’s called, locate a particular pair of socks within a crowded drawer, or decipher between the taste of something that is cinnamon or mint. Challenges with being able to accurately discriminate sensory information can impact one’s capacity to function in their daily lives.
Sensory modulation refers to one’s capacity to respond to and engage with sensory input in an adaptive manner that promotes self-regulation. This includes one’s ability to attend to certain stimuli while ignoring other stimuli (i.e. focusing on your teacher while the birds chirp outside). It also includes how you regulate your arousal level by either engaging with or avoiding sensory stimuli (i.e. listening to music to help you focus or turning off your TV when trying to read).Within Ayres model of sensory modulation there is the concept of:
Sensory Over-Responsivity:
The individual has a low threshold for sensory input; they are hyper aware of sensory information in their environment, or they experience sensory input to higher degree than others.
Sensory Under-Responsivity:
The individual has a high threshold for sensory input; they may not notice and respond to certain relevant sensory input in their environment.
Sensory Seeking (or Craving)
The individual requires a high intensity or frequency of input in order to maintain an optimal level of self-regulation.
Sensory Avoidant
The individual often has a sensory over-responsivity and thus seeks to reduce the amount of sensory in order to maintain an optimal level of self-regulation.
Sensory Processing & Anxiety and OCD
Now how common are sensory processing challenges in people with anxiety, OCD, and related disorders? In a research article published by McMahon et al. (2019), findings showed significant links between early childhood sensory processing challenges and development of anxiety related disorders later into adolescents and adulthood. Children with sensory processing challenges were much more at risk for developing lifelong anxiety related disorders and the relationship between these two variables was mediated by the individuals capacity for emotional regulation.
In 2022, Houghton et al. (2022) conducted a critical review of available evidence on sensory processing and anxiety and OCD. The results found a high prevalence of sensory abnormalities in children with OCD and anxiety related disorders. Finally, in a recent paper published by Cervine (2023), findings showed a high correlation between sensory processing challenges and those with anxiety and OCD. Interestingly, the study highlighted a unique connection between sensory processing challenges and the specific OCD dimension of symmetry/ordering and the specific anxiety dimensions panic and social anxiety.
All this to say, sensory processing and sensory modulation patterns are a critical component to consider in the treatment of many psychiatric disorders, especially those with OCD and anxiety. In addition, occupational therapists and their expert knowledge of sensory processing are in a unique position help integrate the sensory processing framework within current best practices for the treatment of anxiety and OCD (i.e. ERP, CBT, etc.)
Sensory Processing at Mountain Valley Treatment Center
So what does all this mean for how we approach our care at Mountain Valley? How is sensory processing incorporated into individual and comprehensive milieu-based treatment? Read about how the 3 “powerhouse” senses can help with self-regulation here. And stay tuned for next month’s newsletter, where I will discuss in further detail how integrate sensory processing theory into our OT informed milieu.
Sources Cited:
Cervin, M. (2023). Sensory Processing Difficulties in Children and Adolescents with Obsessive-Compulsive and Anxiety Disorders. Research on Child and Adolescent Psychopathology, 51(2), 223–232. https://doi.org/10.1007/s10802-022-00962-w
Houghton, D. C., Stein, D. J., & Cortese, B. M. (2020). Review: Exteroceptive Sensory Abnormalities in Childhood and Adolescent Anxiety and Obsessive-Compulsive Disorder: A Critical Review. Journal of the American Academy of Child & Adolescent Psychiatry, 59(1), 78–87. https://doi.org/10.1016/j.jaac.2019.06.007
McMahon, K., Anand, D., Morris-Jones, M., & Rosenthal, M. Z. (2019). A Path From Childhood Sensory Processing Disorder to Anxiety Disorders: The Mediating Role of Emotion Dysregulation and Adult Sensory Processing Disorder Symptoms. Frontiers in Integrative Neuroscience, 13. https://www.frontiersin.org/articles/10.3389/fnint.2019.00022


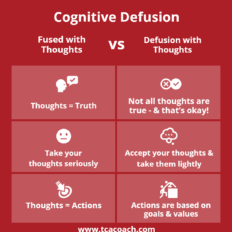 This concept of noticing the thoughts in your head and choosing to observe them rather than engage them, is called cognitive defusion. This ACT based skill is incredibly effective for helping people manage their anxious thoughts in a functional and effective way. With cognitive defusion, the purpose of the skill is to teach people how to live with their distressing thoughts, rather than try to make it go away.
This concept of noticing the thoughts in your head and choosing to observe them rather than engage them, is called cognitive defusion. This ACT based skill is incredibly effective for helping people manage their anxious thoughts in a functional and effective way. With cognitive defusion, the purpose of the skill is to teach people how to live with their distressing thoughts, rather than try to make it go away.




