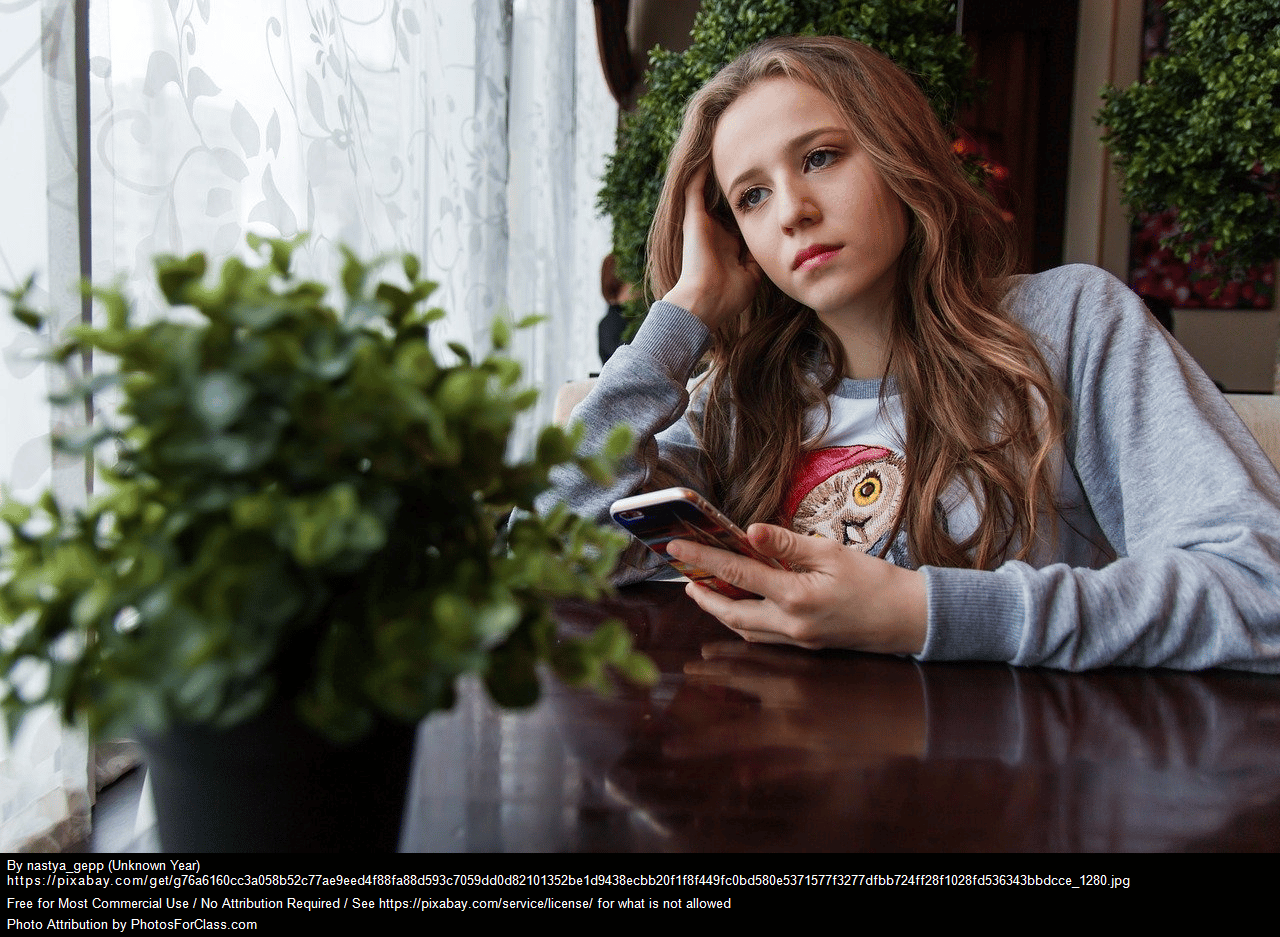
Last spring, the New York Times investigated “Why School Absences Have ‘Exploded’ Almost Everywhere.” The pandemic has dramatically reshaped education in the United States, leading to significant shifts in school attendance and the rise of online learning. According to the Times article, chronic absenteeism among U.S. students has surged since the pandemic, with 26 percent of students now missing at least 10 percent of the school year, nearly double the pre-pandemic rate. This rise in absenteeism spans income levels, racial demographics, and districts, affecting affluent areas and those in poverty alike. Contributing factors include heightened student anxiety, increased illnesses, and a cultural shift that increasingly views school attendance as optional. Schools across the country are now grappling with how to re-establish regular attendance, recognizing that absenteeism hinders both learning and social development.
Simultaneously, online schooling has become a prominent feature of the educational landscape. In 2021, about 74 of the largest 100 U.S. school districts began the school year with remote-only instruction, impacting over 9 million students. Even after the peak of the pandemic, around 75 percent of U.S. schools continue to offer remote or hybrid models, solidifying the role of digital education. In higher education, nearly all universities now offer some form of online classes, with online university enrollment rising by about 11 percent, even as traditional enrollment has slightly declined. For K-12 students, 63 percent use online learning tools daily, highlighting the enduring impact of the pandemic on educational practices.
By allowing children to stay home, parents may unintentionally reinforce the anxiety maintenance cycle, where avoidance becomes a coping mechanism rather than an opportunity for growth. While remote learning provided necessary flexibility during uncertain times, it also became an accommodation that often prevented kids from learning how to push through difficult situations. This normalization of avoidance may offer short-term relief but can ultimately hinder children’s ability to face and manage challenges in the long run. For students struggling with anxiety and chronic absenteeism, avoiding school exacerbates their anxiety, creating a cycle where temporary relief reinforces the fear of school and validates the belief that it is a threat. This avoidance keeps students from engaging in experiences that could help them manage their anxiety, leading to missed academic content, social interactions, and resilience-building activities. As avoidance continues, the anxiety intensifies, particularly regarding returning to school, creating a feedback loop that makes it increasingly difficult for students to confront their fears.
Addressing anxiety is essential for improving school attendance and ensuring students’ success. Online learning options can inadvertently worsen the problem by providing a seemingly safer alternative that reinforces avoidance behaviors. While these options offer short-term relief, they can deepen the struggle with anxiety and create a false sense of security, leading students to believe they are keeping up academically while missing crucial social and emotional aspects of in-person education. This disconnect can lead to further isolation and make reintegration into traditional classrooms even more challenging.
Research underscores the importance of in-person schooling for social-emotional learning (SEL). SEL helps students develop critical skills like resilience, empathy, and emotional regulation, which are best cultivated through direct social interactions in classrooms, group activities, and extracurriculars. Meta-analyses show that in-person learning positively impacts students’ social, emotional, and academic outcomes. These programs are particularly effective when integrated into the school environment, where active, consistent engagement is possible. Additionally, in-person schooling offers opportunities for students to build relationships with peers and adults, fostering a sense of belonging and emotional safety—elements that are harder to replicate in online environments. The community and connection found in schools are essential for students’ overall development, making in-person education crucial for their growth.
In-person schooling also significantly contributes to career success by fostering a range of valuable skills and experiences. Face-to-face interactions help students build essential interpersonal skills necessary for networking and effective communication in the workplace. Immediate feedback from teachers teaches students to handle constructive criticism and adapt quickly, skills that are valuable in professional settings. The structured environment of physical schools promotes time management and organizational skills, aiding students in managing professional responsibilities. Hands-on learning opportunities, such as practical experiments and group projects, provide real-world skills that are highly valued in many careers. Access to resources and extracurricular activities offers additional opportunities for skill development and career exploration. Emotional support from teachers and counselors builds resilience, helping students handle workplace stress and challenges. The community and networks established during schooling provide valuable connections and support throughout one’s career. Familiarity with technology and troubleshooting skills gained in school also prove beneficial in today’s tech-driven workplaces. Together, these aspects of in-person education create a strong foundation for career success, complementing individual skills and experiences.
The rise of online learning and the increase in chronic absenteeism have introduced complex challenges for educators and students alike. While online education offers flexibility, it often reinforces avoidance behaviors in students with anxiety, deepening their struggles and stunting their personal growth. To combat this, effective anxiety treatment must be prioritized, addressing the root causes of avoidance rather than merely accommodating it. By focusing on interventions that help students manage their anxiety and confront their fears, schools can improve attendance and ensure that students fully benefit from the in-person education experience. As educators continue to navigate these challenges, prioritizing anxiety treatment and re-engaging students in traditional school environments will be essential for their long-term success.



 Last week, on the Fear Less Podcast, we released Episode #36: “Fear, Fatherhood, and Transformation: Zack’s Journey to Becoming Dad.” In this episode, I reflected on the biggest life transition I have made to date—becoming a father. In my reflection, I talk about the role fear and anxiety played throughout my journey into fatherhood, and how impactful my fear was in helping me refine who I am and who I wanted to be as a father.
Last week, on the Fear Less Podcast, we released Episode #36: “Fear, Fatherhood, and Transformation: Zack’s Journey to Becoming Dad.” In this episode, I reflected on the biggest life transition I have made to date—becoming a father. In my reflection, I talk about the role fear and anxiety played throughout my journey into fatherhood, and how impactful my fear was in helping me refine who I am and who I wanted to be as a father.
 Although the impact of social media and technology on mental health, especially youth, has been in question for some time, it has become quite the “hot topic” in the public media recently. Approximately one year after issuing a
Although the impact of social media and technology on mental health, especially youth, has been in question for some time, it has become quite the “hot topic” in the public media recently. Approximately one year after issuing a